
![]()
0 hours
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
0.5 hours
These are activities that require reflection on feedback about your work.
![]()
0 hours
These are activities that use your work data to ensure quality results.
![]()
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
These are activities that require reflection on feedback about your work.
![]()
These are activities that use your work data to ensure quality results.

A 36-year-old female attended review with her GP after self-detecting a right breast mass. She denied any other breast concerns. On examination, she looked well and had a BMI of 27. Her clinical examination identified a 1cm right retroareolar mass without any palpable right axillary lymphadenopathy.
Breast cancer (paternal grandmother, age unknown).
A right breast ultrasound was arranged. In the patient’s area of concern, a 13mm lobulated hypoechoic lesion was seen at the right retroareolar position. Additionally, there was an incidentally detected 4mm spiculated, hypoechoic lesion at the right breast at 2 o’clock 2cm from the nipple. This had indistinct outlines, acoustic shadowing and associated vascularity.
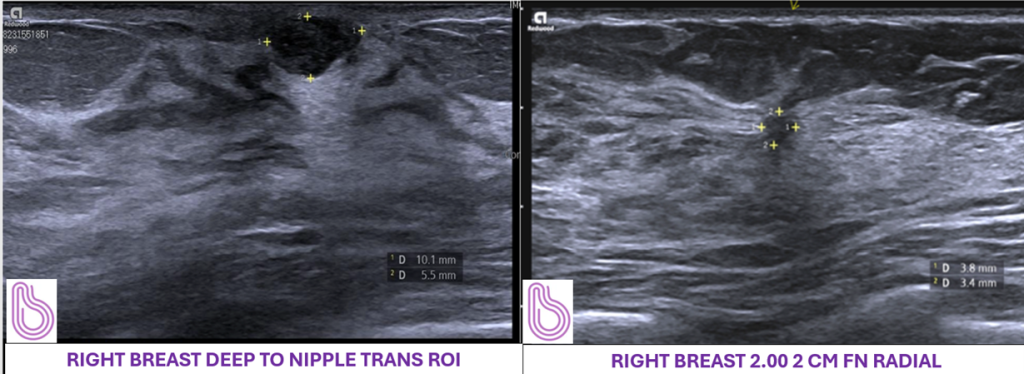
The presenting area of concern had benign imaging characteristics and was consistent with a fibroadenoma. The 2 o’clock lesion however was reported to have BI-RADS 4c imaging characteristics, and the radiologist discussed their concerns with the referring GP.
The patient was reassured of the benign pathophysiology of fibroadenomata, and that these could be monitored with progress imaging. However, further investigation of the 2 o’clock lesion was recommended to complete their breast assessment. This included considerations for bilateral breast imaging for a thorough assessment, and supplementing her mammogram with contrast to improve the sensitivity of the mammogram given the anticipated breast density in a young woman.

As the benign histology result was not concordant with the imaging findings, further assessment options were discussed. This included vacuum-assisted biopsy, breast MRI or diagnostic breast surgery. As per her preference, the patient proceeded to a diagnostic excisional biopsy of the lesion. Surgical histology confirmed the lesion as a radial scar with no evidence of malignancy.
Given the lesion was benign, no further treatment was recommended for the 2 o’clock lesion. The patient was advised to repeat ultrasound imaging in 12 months to assess stability of the lesion, and to undergo slightly-above population risk breast cancer screening with biennial mammography when she is 50 years of age.
*Model of Care at Breast Imaging Victoria: A multidisciplinary team is on-site to provide comprehensive, holistic and personalised breast care to all patients.
The choice and benefits of different breast imaging modalities may be nuanced and benefit from discussion with a dedicated breast radiologist. A patient-centred, multidisciplinary approach will provide personalised and improved patient care.
Case study provided by Breast Imaging Victoria. Reviewed by Dr Eugenia Ip (specialist breast surgeon) and Dr Charuta Dagia (breast radiologist).
Based on this educational activity, complete these learning modules to gain additional CPD.




Browse the latest articles from Healthed.

















