
![]()
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
These are activities that require reflection on feedback about your work.
![]()
These are activities that use your work data to ensure quality results.
![]()
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
These are activities that require reflection on feedback about your work.
![]()
These are activities that use your work data to ensure quality results.

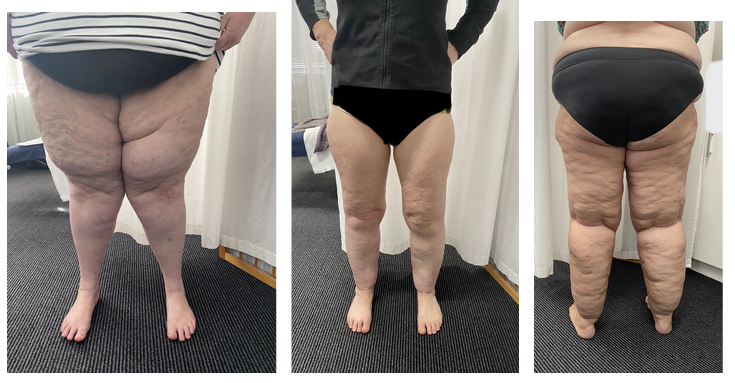
While often mistaken for obesity or lymphoedema, lipoedema is a distinct condition that needs to be managed differently. There are key signs and symptoms to look out for—and recognising it early could help reduce the risk of consequences such as disordered eating, depression and osteoarthritis.
Lipoedema is a chronic disorder that almost exclusively affects women. It involves an abnormal, bilateral accumulation of subcutaneous fatty tissue predominantly in the thighs and buttocks—although it can occur in the arms, abdomen and other parts of the body.
Its cause is not known but genetic and hormonal factors are thought to be involved.
Lipoedema can have a significant emotional impact, with some data suggesting affected patients have a high prevalence of mental health disorders, says Lucy Melican, a lymphoedema physiotherapist and Lipoedema Australia board member.
It can also impair mobility and everyday function.
There is no cure, but treatment can help ease pain and oedema, improve quality of life and slow progression.
In 2019, the World Health Organization recognised lipoedema as a distinct condition and gave it an ICD-11 code.
Although little is known about lipoedema, “It’s not just that people are overweight,” stresses Melbourne-based endocrinologist Dr Rosie Worsley.
“The fatty tissue in lipoedema does seem to be different to normal fatty tissue,” she says, citing an Australian study that found significant differences in key cellular signalling pathways in tissue from patients with lipoedema compared to that of unaffected controls. “That kind of biological data is pretty convincing.”
Ms Melican emphasises that “lipoedema fat is completely different fat to obesity. It is not obesity and does not respond to the same management strategies as obesity.”
Lipoedema has nothing to do with “a lack of motivation, poor eating habits or laziness on the part of the sufferer,” she says.
“Lipoedema fatty tissue grows due to genetic and hormonal signalling, not due to lifestyle factors.”
“Later in life, as the patient becomes more confused, distressed and disenchanted and often after trying many extreme diets, they may gain more ‘normal’ fat due to giving up as nothing works, and often due to a reduction in comfortable mobility impacting their ability to exercise.”
Global consensus about diagnostic criteria is yet to be reached, Ms Melican says, but some countries have developed their own lipoedema guidelines, including the United States and the Netherlands.
Lipoedema’s prevalence is not known and population estimates vary.
A small but robust German study found a prevalence of 39%, Ms Melican says, with approximately 10% having “quite significant symptoms”, while an assessment conducted by Lipoedema Australia suggested a prevalence of 19%.
“The problem we have though with defining population data is that we do not have an agreed upon, clinically reproducible criteria for diagnosing it. There’s no clinical biomarker, there’s no definitive symptom combination. So we’re actually basing these numbers on the skill of the assessor or the knowledge or the general consensus at that point.”
Diagnosis is further complicated by the “huge range in clinical presentation,” Ms Melican says. “It’s very variable. Sometimes it could be quite a mild version.”
There are key things to look out for, however.
Two key symptoms are highly indicative of lipoedema, Ms Melican says.
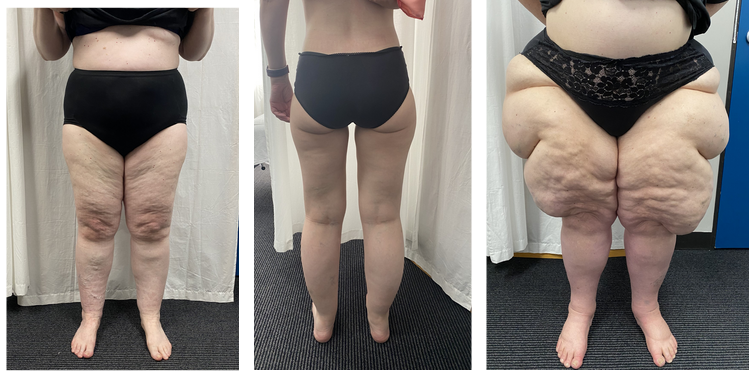
Despite lack of agreement over diagnostic criteria, there is consensus that lipoedema involves body disproportion, “with the lower body being heavier than the upper body,” Ms Melican says.
A telltale sign is that when patients lose weight, it often comes off their trunk, “but their legs and thighs stay quite heavy, even though they might have lost 10 kilos. Or they do a boot camp with their friends and everyone loses five kilos, but they lose one kilo and it’s only around their waist.”
The disproportion usually emerges after puberty but can develop at other times of hormonal or body shape change.
“It can come on during or after pregnancy or after menopause and tends to get worse with age,” Dr Worsley says. “But we don’t really know why or how that works.”
“They’ll often report symptoms like my legs feel heavy, like I’ve got cement boots on, like I’m wading through honey or lugging lumps of wood,” Ms Melican says.
“All these sorts of phrases indicate that their legs don’t feel right and that they’re more aware of their legs than the rest of their body.”
They might also report:
Observation and palpation provide crucial pointers, Ms Melican says.
“You’ll see a classic dimpled appearance that you often see on women around the upper thigh and buttock, but they tend to have it widespread over their entire thigh and sometimes on their calf.”
Fatty pads around the knees are common: “Not everyone has them but it’s particularly non-anatomical,” Ms Melican says.
“They often stand with slightly valgus knees and sometimes slightly hyperextended as well, and often have pronated feet,” she adds.
She recommends palpating the leg medially from the upper calf to lower thigh.
“If you walk your fingers over that area, you’ll often feel nodular fatty tissue. It doesn’t feel smooth and rubbery like normal fat,” she says. “Not in 100% of cases but in probably 90%.”
That area is often tender, even if you can’t feel any nodules, she adds.
“The lateral and anterior thigh are often tender as well, but I just find that medial area is most likely to be tender.”
Some experts think pain should be a definitive diagnostic criterion but Ms Melican disagrees, noting it is subjective, not always present, and difficult to test—with no consensus about how to assess it.
It can be more helpful to ask patients if they have altered sensation in affected areas, she says, such as heaviness, throbbing, tightness, dragging or drawing.
Many lipoedema patients have an elevated BMI, but they are more likely to have normal metabolic markers than those with obesity, she says.
Measuring waist to height ratio can help differentiate between lipoedema and obesity, especially if BMI is elevated, she adds, because people with lipoedema who are not overweight or obese are less likely to have central adiposity.
Their blood pressure is also often lower than expected.
The cause is not known so “we’re not looking for any specific things,” Dr Worsley says.
She recommends running standard screening bloods, noting the rate of diabetes in lipoedema patients is “pretty low.”
Lipoedema is under-recognised and women can wait years to be diagnosed, with research showing they often experience fat-shaming, self-blame, and feelings of being controlled by a burdensome body.
Many patients have repeatedly been advised to lose weight, with failure leading to frustration and feelings of futility.
“Recognising and understanding the condition and giving them an alternative option apart from losing 10 kilos can make the biggest difference to patients,” Ms Melican says. “Once you explain what is happening and why, the relief and the psychological benefit from that is absolutely massive.”
Dr Worsley says that “If you take people seriously, they do feel very validated but also they can then take some proactive steps that help with their quality of life.”
Diagnosis can also help stave off other adverse impacts, Ms Melican notes.
“The prevalence of conditions like anorexia is really quite high in lipoedema,” she says. “You could short circuit something like that if they understand what’s happening, rather than thinking ‘My friends can all have skinny legs, why can’t I? Something’s wrong with me—I need to stop eating’.”
Lifestyle measures to reduce inflammation—such as healthy eating, supplements, improved sleep, and stress-relieving strategies—can all help, Ms Melican says.
GPs can also deal with other issues patients report, such as knee pain.
Exercising in the pool is often helpful and an easy thing to recommend, she says, “The cruel irony is that it means a person who doesn’t like their body has to get into swimwear, but we often suggest they get a cheap pair of leggings and just pop them over their bathers.”
Weight loss treatments will not ‘fix’ the lipoedema deposits but are worth trying if the patient has co-morbid obesity, Dr Worsley says.
Drugs such as semaglutide (Ozempic or Wegovy) and tirzepatide (Mounjaro) can be helpful, she says.
“They seem to take longer to work in lipoedema patients, but they do often get some benefit. They might get a small amount of weight loss. Interestingly, a lot of them find their legs hurt less.”
“And that’s just anecdotal. There are no randomised controlled trials at all.”
Ms Melican believes weight loss drugs are probably best prescribed only if metabolic markers are elevated or patients have significant pain.
Dr Worsley says bariatric surgery may also be an option.
Ms Melican suggests referring patients who are distressed or report symptoms that impact their quality of life—such as their sleep or movement—to a lymphoedema therapist who treats lipoedema.
Find Australasian Lymphology Association-accredited practitioners on the National Lymphoedema Practitioners Register.
Patients can develop osteoarthritis at an early age and referral to a musculoskeletal physio might be appropriate, she adds.
Dr Worsley says referral to an endocrinologist or obesity expert may be helpful for weight management. She notes surgical debulking such as liposuction may be necessary in patients experiencing significant mobility impairment.
Ms Melican says surgery can also be considered if symptoms are not adequately managed after a year or two of conservative therapies. She advises referring to a plastic and reconstructive surgeon experienced in lipoedema management.
A recent systematic review and meta-analysis concluded that liposuction is safe and can improve lipoedema symptoms and quality of life.
Based on this educational activity, complete these learning modules to gain additional CPD.



Browse the latest articles from Healthed.











")


