

Two out of five Australians have tried unsuccessfully to get off antidepressants, according to Dr Mark Horowitz, co-author of the recently released Maudsley Deprescribing Guidelines.
Dr Horowitz says severe withdrawal symptoms are underestimated by the medical profession, and guidance for antidepressant cessation has historically not been based on any empirical evidence.
The Therapeutic Guidelines recommend reducing the dose by 25 to 50% every one to four weeks until the daily dose is half the lowest unit strength available, then continuing at the lowest dose for two weeks before stopping, but he is critical of this approach.
“We have surveyed people including in Australia and this is the most common way that people have been taken off antidepressants – reducing by half for two weeks and reducing dose to a quarter for two weeks – often by alternating half a tablet every second day,” he said in a recent public lecture hosted by the Australian Society for Psychological Medicine.
He points to a randomised controlled trial that found just 6% of people were able to stop their antidepressant this way: “so it’s generally not a very successful method.”
As a consequence, “hundreds of thousands of people have exited healthcare and gone onto online forums to get advice on how to come off the medication.”
Psychiatrist and suicide prevention advocate Professor David Horgan believes the risk is being overstated.
“I personally have prescribed and changed SSRIs and SNRIs over 10,000 times. I have seen only one patient who could not stop them, she reported,” Professor Horgan said.
“I did a survey of 400 Australian psychiatrists a few years ago which showed their impression that 30% of patients had some withdrawal symptoms…this is a far cry from being unable to stop,” he added, noting that when tapered appropriately, withdrawal symptoms become much less likely.
Dr Horowitz says that for 20 years, guidelines based on eight-to-twelve-week studies run by drug companies said that withdrawal symptoms are only mild and brief, but they are far more common and severe than previously thought— and UK guidelines have changed to reflect this.
“Of the three million Australians on an antidepressant, approximately half will have some trouble. How much trouble depends on which drug and for how long [they have been on it].”
A 2018 review of 14 trials found more than half of patients experienced withdrawal symptoms, and 46% of them reported their symptoms were ‘severe’, Dr Horowitz said.
He stresses these symptoms occur due to neurological ‘adaptation’ to the drug and not addiction, which would be characterised by additional symptoms such as compulsion and cravings.
And while patients are often told they cannot have prolonged withdrawal symptoms because the drug leaves the system in days or weeks, synaptic changes can take up to four years to ‘reset’ following antidepressant cessation, Dr Horowitz said, so withdrawal symptoms can sometimes last for months or even years.
However, Professor Horgan again disputes the claim that serious or extended withdrawal symptoms are common when patients taper off antidepressants.
“Withdrawal reactions are very rare in my experience if one reduces the dose 25% every three or four days. Many psychiatrists cross taper antidepressants without waiting for total washout,” Professor Horgan said.
Psychiatrist and Professor Mal Hopwood agrees. Most clinicians — GPs and psychiatrists alike — feel it is not as frequently severe as the authors suggest, he said.
“Part of the reason the debate persists is that the studies of the accrual frequency tend to be limited and/or imperfect,” Professor Hopwood explained.
Although that debate is not yet settled, it’s clear that some patients do experience withdrawal symptoms, and it’s important to be able to identify them and take steps to reduce them.
In a March Healthed survey, 48% of GPs said they were either only ‘somewhat confident’ or ‘not at all confident’ in their ability to distinguish between antidepressant withdrawal symptoms and symptoms of depression recurrence. Just 10% of 2253 GPs rated themselves as ‘very confident,’ while 42% were ‘moderately confident.’
Both patients and doctors can find it difficult to differentiate between withdrawal symptoms and symptoms of relapse, said Professor Katharine Wallis, Head of the Mayne Academy of General Practice at the University of Queensland Medical School and lead of the RELEASE (REdressing Long-tErm Antidepressant uSE in general practice) study.
But there are signs to look out for.
“If you’re going to get a relapse of some sort of major condition, that tends to come on over a period of weeks or months, whereas withdrawal symptoms tend to come on more quickly after stopping antidepressants or decreasing the dose,” Professor Wallis said.
“Also, withdrawal symptoms are very quickly relieved by going back on the drug. Within a few days or a week people will be feeling the symptoms are gone and we know that for major depressive disorder it takes longer to get a treatment effect.”
Dr Horowitz said antidepressants affect multiple body systems, so symptoms on stopping or reducing the dose can be wide-ranging.
The most common withdrawal symptoms are:
One study documented an increase in suicide attempts in the two weeks following antidepressant cessation.
Another troubling yet often overlooked symptom is akathisia, which is generally recognised as a side effect of long-term antipsychotic drug use but can occur in withdrawal from anti-depressants, Dr Horowitz said.
While many symptoms of withdrawal and depression overlap, Professor Wallis and Dr Horowitz advise looking out for distinguishing symptoms such as dizziness and brain zaps, as well as any symptoms that were not present in the baseline condition.
Professor Wallis and Dr Horowitz both say that stopping antidepressants abruptly can be dangerous.
“In my mind, it’s the equivalent of jumping off the top of a 10-story building,” Dr Horowitz said. “It’s the quickest way to cause destabilisation of someone’s homeostasis.”
Moreover, the typical linear approach to dose reduction “starts off like a gentle country decline, turns into a steep hill and then becomes a cliff which people fall off,” he said.
Instead, Dr Horowitz advises a “hyperbolic tapering” approach, which studies have shown reduces both relapse rates and the risk of withdrawal effects.
“That requires doses that get smaller and smaller…down to extremely small final doses before stopping,” he said, adding that some people can only taper by as little as 10% of their last dose per month.
He said the Royal College of Psychiatrists have released guidance on ‘Stopping antidepressants’ which recommends:
Draft NICE guidelines have adopted the same guidance, Dr Horowitz said.
Dr Horowitz said you can start off using tablet cutters to divide tablets into halves and quarters.
Liquid preparations make things easier, but escitalopram is the only antidepressant available as a liquid in Australia.
Compounding pharmacies can make up liquids, tablets or capsules, he said.
Skipping doses is not a good idea except for fluoxetine, he said, because most anti-depressants have a half-life of less than 24 hours.
“If you take a drug every second day, you’ll have a quarter of peak levels by the end of the second day and that can for many people precipitate withdrawal symptoms.”
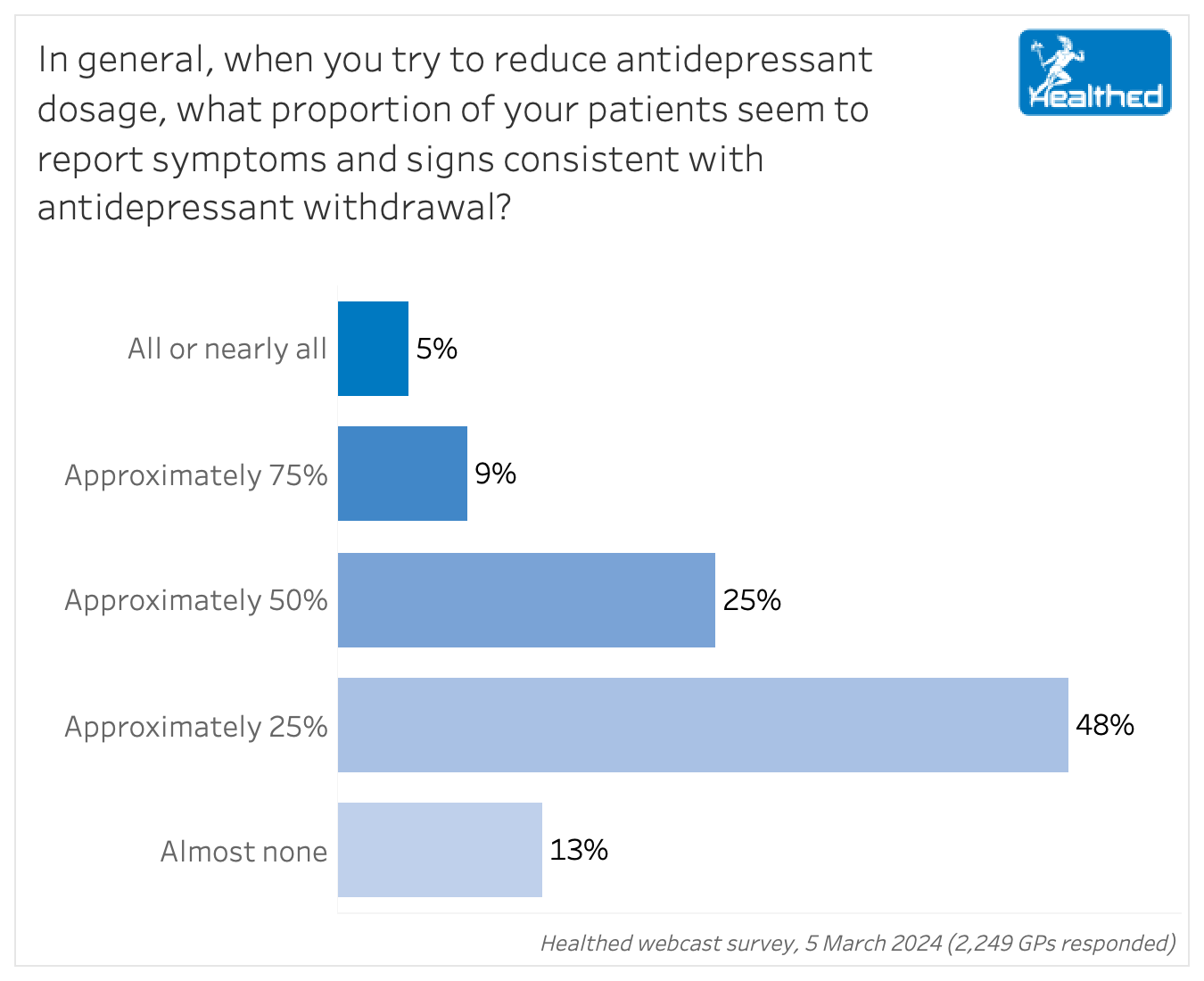
How often do GPs encounter antidepressant withdrawal in practice?
While GPs in Healthed’s March 2024 survey differed substantially in their confidence in distinguishing withdrawal symptoms from relapse, they also varied widely in their assessment of the proportion of patients who experience withdrawal symptoms when coming off antidepressants.




Browse the latest articles from Healthed.
















